Male Infertility
Azoospermia
(Obstruction of the male reproductive tract)
The lack of sperm in the ejaculate (azoospermia) can occur as a result of impaired production or blockage (obstruction.) Obstruction can be acquired (after infections, vasectomy or other surgery that can cause a blockage) or congenital – something you are born with. One of the most common causes of congenital obstructive azoospermia occurs when men are born without the vas deferens (and usually a large section of the epididymis, that is where sperm normally go just outside of the testis.) This is referred to as congenital bilateral absence of the vas deferens. This congenital condition is most commonly caused by mutations in the cystic fibrosis (CF) gene, so testing of the female partner to assure that she is not also a carrier for CF is important (since 4-5% of the US population are CF gene mutation carriers.) Another subset of men with congenital absence of the vas have an abnormal kidney, so renal/kidney ultrasound may be done for infertile men with this condition.
Microsurgical reconstruction of obstruction
For men with acquired obstruction, microsurgical reconstruction (vaso-vasostomy or vaso-epididymostomy) may be done to fix the problem and allow couples to have child naturally. Alternatively, sperm retrieval can be done to allow the sperm to be used with assisted reproduction (IVF/ICSI.) Sperm production is typically normal, so sperm can be retrieved from the testis, epididymis, or even the vas deferens, if present.
Sperm retrieval can be done with a needle procedure under local anesthesia, or tens of millions or even more sperm with the best quality, can be retrieved with a simple surgical procedure called microsurgical epididymal sperm aspiration (MESA.) The epididymis has at least 10 different segments, each of which has slightly different sperm quality. With MESA, each of these sites can be sampled, and the best sperm quality then used for IVF. With use of epididymal sperm, we have observed the highest pregnancy rates of almost any subset of couples treated with IVF (https://pubmed.ncbi.nlm.nih.gov/10221707/., https://pubmed.ncbi.nlm.nih.gov/11020509/.)
The MESA procedure was refined at our center many years ago ( https://pubmed.ncbi.nlm.nih.gov/8833735/ )and continues to be used effectively to limit the number of procedures needed for a man, still providing the best sperm quality that could be used for IVF to allow couples to have as many children as they would like to have.
Sperm retrieval with percutaneous testis biopsy also provides limited numbers of sperm with a less invasive procedure, but repeat procedures may be needed for additional IVF tries, there is a higher complication rate (bleeding) with percutaneous procedures, and lower success rates are typically seen with IVF using testicular sperm.
Azoospermia: Non-obstructive azoospermia
Non-obstructive azoospermia, where no sperm reach the ejaculate because of impaired sperm production, is considered the most severe form of male infertility. Evaluation of men with this condition requires hormonal evaluation as well as genetic testing to best predict the prognosis for successful treatment and to identify conditions, such as low testosterone, that can be treated to optimize sperm retrieval. Dr. Schlegel has published multiple medical journal articles that identify how to best evaluate for and interpret genetic conditions ( https://pubmed.ncbi.nlm.nih.gov/11148736/ ), to optimize hormonal status ( https://pubmed.ncbi.nlm.nih.gov/22179517/ ) and provide the most effective surgical treatment for sperm retrieval ( https://pubmed.ncbi.nlm.nih.gov/19247918/, https://pubmed.ncbi.nlm.nih.gov/23241638/) An overview video for treatment of non-obstructive azoospermia is provided here ( https://youtu.be/yoaf0–up6s?list=TLPQMjEwOTIwMjP1bcMbSy7Ktw )
In addition to providing the refining and providing the best results for men with non-obstructive azoospermia, Dr. Schlegel has taken steps to optimize using even rare sperm from the ejaculate for men with severely impaired sperm production ( https://pubmed.ncbi.nlm.nih.gov/37517636/). This is a critical differentiating distinction between the care we provide and that available at other centers. Although it takes extra work for a reproductive urologist as well as the IVF laboratory to use the rare sperm present in the ejaculate, it allows couples to often be treated without surgery. If your reproductive team has recommended surgery and you did not have the opportunity to provide another semen sample during IVF, consider further evaluation of your care. We find that 9.6% of men with presumed non-obstructive azoospermia who are scheduled for surgery can avoid that surgery if another semen sample is obtained on the day of planned sperm retrieval, as we routinely do. Details are provided in this video ( https://youtu.be/0WaTfxB6IeA?list=TLPQMjEwOTIwMjP1bcMbSy7Ktw )
We have described our approach for treatment of non-obstructive azoospermia and IVF in a series of different medical publications ( https://pubmed.ncbi.nlm.nih.gov/36301052/, https://pubmed.ncbi.nlm.nih.gov/28904907/) and the guidelines for management of male infertility produced by the American Urological Association and the American Society for Reproductive Medicine ( https://pubmed.ncbi.nlm.nih.gov/33295257/, https://doi.org/10.1016/j.fertnstert.2020.11.016 )
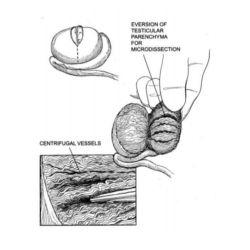
Figure: The demonstration of individual seminiferous tubules within the testis is schematically shown, including the parallel relationship of the centrifugal blood vessels of the testis that run parallel to the seminiferous tubules that can contain sperm.
Non-obstructive azoospermia is best treated with microTESE together with IVF ( https://pubmed.ncbi.nlm.nih.gov/26263080/ ). Sperm retrieval techniques such as FNA mapping are not as effective in comparative trials as microTESE, and FNA mapping must be followed up with surgery to actually provide enough sperm for IVF. Our personal experience is that FNA mapping often misses the best sites of sperm production in the testis. When we have operated on men who previously had FNA mapping, we typically find that the “map” has missed the best sites of sperm production that we find with the detailed search of testicular tissue that is possible under an operating microscope with the microTESE procedure. Video description of the microTESE procedure is provided here ( https://youtu.be/s8NK_33638E )
Consult with Dr. Schlegel
Take the first step towards better health and schedule a consultation with Dr. Schlegel today to discuss your specific concerns and explore personalized medical solutions.